- About Us
- Ilizarov Technique
- Process
- Case Studies
Fractures
• Acute Fracture - Comminuted Fracture Distal Humerus - Compound Fracture & VAC • Nonunion - Proximal Tibia - Tibia - Distal Humerus • Malunion - Femur Bone Deformity
• Acute Correction
- LRS - Bilateral Tibia - LRS - Rotational Deformity Femur(with Shortening) - LRS - Oblique Plane Deformity Femur - Nailing • Ilizarov Correction - Proximal Tibia - Distal Femur • Hexapod Correction - Metaphyseal Dysplasia Bone Infection
• Infection - Femur • Infected Nonunion - Proximal Femur Joint Problems (Arthritis)
• Hip Replacement • Knee Replacement • Intra Articular Osteotomy • High Tibial Osteotomy (HTO) • Arthrolysis - Elbow • Ilizarov Hip Reconstruction - FAQs
- Testimonials
News & Updates



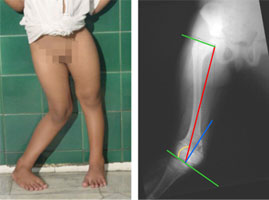
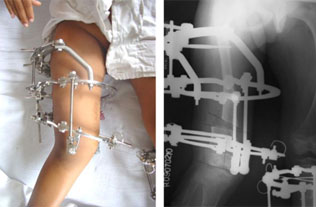
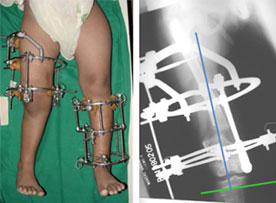
Ilizarov Correction - Distal Femur
|
||
| The blue line marks the normal angle of the distal femur to the knee joint. | ||
|
||
|
||
|
||
| The scars seen are the sites of pin insertion. The actual incision for cutting the bone is about 1-1.5 cm and requires just two sutures. With time even these pin site scars become lighter. | ||