
- About Us
- Ilizarov Technique
- Process
- Case Studies
Fractures
• Acute Fracture - Comminuted Fracture Distal Humerus - Compound Fracture & VAC • Nonunion - Proximal Tibia - Tibia - Distal Humerus • Malunion - Femur Bone Deformity
• Acute Correction
- LRS - Bilateral Tibia - LRS - Rotational Deformity Femur(with Shortening) - LRS - Oblique Plane Deformity Femur - Nailing • Ilizarov Correction - Proximal Tibia - Distal Femur • Hexapod Correction - Metaphyseal Dysplasia Bone Infection
• Infection - Femur • Infected Nonunion - Proximal Femur Joint Problems (Arthritis)
• Hip Replacement • Knee Replacement • Intra Articular Osteotomy • High Tibial Osteotomy (HTO) • Arthrolysis - Elbow • Ilizarov Hip Reconstruction - FAQs
- Testimonials



HTO
Osteoarthritis of the knee is a troublesome and disabling disorder. A few years ago, there were not very many options other than arthroplasty (joint replacement) for knee pain. Joint replacement for osteoarthritis is the ultimate treatment option even now, but only for those who are above 60 years of age and for those who are not going to put lot of load on the artificial joints.
For a young patient of less than 60 years, or a very active person or a person involved in demanding sports, who has pain in the knee joint, especially on walking or prolonged standing and is beginning to loose the cartilage cushion in the knee on x-ray, the High Tibial Osteotomy (HTO) is the procedure which adds life to the knee.
When the cartilage cover is lost, bones of the knee joint start to grind on each other giving rise to pain and overloading one side of the joint. The general tendency is to ignore the pain or take painkillers and continue with the daily activities. As this goes on, the knees get worn out and then there is nothing much left to do other than a joint replacement. But if tackled in the initial stages by HTO one gets complete relief from pain, the degenerative process slows down and one can lead a healthy and active lifestyle. Once HTO is done, depending on the initial damage a joint replacement surgery can be postponed either by about 15 years or may not require a knee replacement altogether.
In HTO, the tibia is cut through 1cm incision and straightened. The bone is fixed using either an external fixator or a bone plate. The fixator assists in gradual and accurate correction of the bone in the postoperative period whereas the plate helps to maintain the correction achieved immediately in the surgery. The hospital stay is about 5 days and the procedure is virtually painless. The load distribution of the joint is corrected and the degeneration slows down. The joint space also becomes normal with time as the cartilage “grows back.”
This is similar to wheel balancing; when the tyres are not in alignment what they need is correction of alignment and not replacement. Similarly when the malalignment of the leg is tackled by this kind of procedure the balancing of natural knee is achieved with good results.
High Tibial Osteotomy is not a new procedure. It has been described in medical literature from as early as 1950s. The procedure described was a closing wedge osteotomy, where a wedge of bone was removed from the upper tibia (leg bone close to knee) and upper fibula (smaller leg bone next to tibia). This would change the shape of the bone and therefore cause difficulties in future knee replacement surgery. This is the reason that HTO is not the preferred treatment modality in the minds of many Orthopedic surgeons. Another reason that is often told to the patient is that the results last for only 5-7 years.
At the Center for Limb Lengthening & Reconstruction, Mnagal Anand Hospital, Mumbai, we are dedicated to revive the art of osteotomy & its benefits. HTO at our center is performed using minimally invasive open wedge technique. The gap which is created by the open wedge gradually fills up with new bone naturally. Since bone is not excised, the shape of the bone is not changed, therefore no complications for a future knee replacement if required. Studies have been done and are still ongoing regarding the benefits of a properly done HTO. They have all proven that if the angle is corrected within a narrow margin of 3-5∘then the results can last 15 years or more. To achieve such an accurate correction we recommend the use of an external fixator which allows us to fine tune the correction to a degree and guarantees good and long lasting results.
There are other methods for assisting the open wedge technique of HTO performed at the Center for Limb Lengthening & Reconstruction, Mnagal Anand Hospital, Mumbai. These methods are:
- The Tomofix type of internal fixation (a locking plate which is applied on the inside - thereby nothing is seen from outside)
- Hexapod Fixator (an external fixator with rings and a six-axis correction system). There are advantages and disadvantages to each method and these can be discussed in detail at the time of consultation.
| An example of correction of a uniplanar deformity in the proximal tibia. |
| The picture on extreme left shows that the patient had varus deformity of the proximal tibia i.e. bow legs (reduced angle at the bone close to knee) on both the sides, with the mechanical axis of the lower limbs (load bearing axis from the hip to the ankle) passing on the inner side of both the knees (normally the line should be passing from the center of the knee). |
| The picture second from left shows the post surgery status about 4 weeks after surgery (High tibial Osteotomy using an Orthofix fixator). The deformity has been corrected by gradual distraction of 1mm per day. The patient is walking with the aid of a pair of axillary crutches. |
| The picture on the extreme right shows the actual incision of about 1.25cm made for the percutaneous osteotomy (minimally invasive technique for cutting the bone). |
| The picture second from right was taken 2 weeks after fixator removal. The left side shows excellent correction as compared to the right side, which is yet to be operated. |
 |
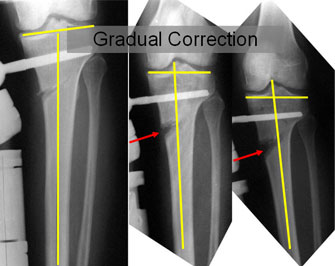
| The xray pictures during the gradual distraction process of high tibial osteotomy. |
| The picture on the left is taken after surgery, before the distraction is begun. The distraction is started 5-7 days after surgery. This helps in initiation of the healing process and better formation of regenerate. The lines drawn show the angle between the joint line of tibia and the anatomic axis of tibia. The inner angle is reduced in this case. |
| The picture in the center shows an increasing gap at the osteotomy site (marked by arrow). With the increase in the distraction gap the inner angle is also increasing. |
| The picture on the right side is taken at the completion of the distraction process, the gap at the osteotomy site(marked by arrow) has opened up sufficiently, the inner angle has increased to the required amount. |
 |
| The final result as shown in the clinical pictures, full length x-ray and spot film of the knee. |
| The full length x-ray (second from right) confirms the mechanical axis is central again on the left side whereas the unoperated side axis is passing medial to the knee. |
| The spot film (extreme right) confirms a 5º femoro-tibial valgus angle (normal femoro-tibial angle is 3-5º). |
 |